


ADHD: Steroids, The Gym, and The Game
Asking questions about amphetamines, meditation, and the neuroscience and phenomenology of attention.

Ok, I promise I’m going to talk about ADHD soon (if I remember), but first let’s talk about body-building. While generally pretty lean, I’ve weight-lifted off and on for many years. It’s a super-efficient way to get exercise in the office, and it’s good for balancing the surfing. As such, I’ve watched a lot of diet and gym bro YouTube. And man, there is a lot of commentary flying around about juicing (steroids) versus natty (natural). There’s proud natty influencers, and there’s honest-and-thoughtful juicers, but everyone agrees that the game is changing. Steroids have side effects, but they work, and they are becoming increasingly popular.

The natty influencers talk about how it’s harder and harder to compete for attention without taking steroids themselves. For an informal competition like “being a well-known YouTuber”, there are no rules. (although there are many ways to skirt the rules for actual competitions) So for that game in particular, steroids are becoming more and more a necessity.
Now Look Here
Switching gears again. Lately, I’ve been paying a lot of attention to attention. While my grad-school self was more interested in sensory encoding models than the neural mechanisms of attention, meta-cognition about my own attention is not a particularly new interest for me. For many years, I have been annoyed by what I considered my “distractability”, or “procrastination”. Why, so frequently, have I caught myself paying attention to something that isn’t what I “should” (want to?) be paying attention to? Is something broken? Is it natural? Managing my attention is something that I’ve worked with, and found ways around. I remember telling one of my more productive coworkers some of the mental games and coping strategies I have developed to be able sit at a desk for enough hours to have a career in our culture, and watching his eyes grow wider and wider. If I were telling the story that I call the “standard mental-health victory story”, I would go on to say I sought out mental health consultation and learned, to great emotional catharsis, that it wasn’t my fault. (it was just ADHD!) I’d have gotten a prescription for amphetamines, and realized a significant productivity boost. I would then give a heart-felt advocacy of reaching out for help, with the clear implication that the correct place to seek help is with “professionals” aka, the establishment psychiatric care system.
Well, I’m not going to tell the standard mental health victory story. It is not that I have never sought out help for my mind. I’ve never really had the “men don’t need help” American cultural hangup, and I have always been interested in maintaining a healthy body, mind, and spirit. Over the course of my life I’ve sought help for various issues from therapists, counselors, friends, mentors, coaches, mystics, and Dharma teachers. Although I certainly match enough of the DSM-V criteria to acquire an ADHD diagnosis if I want one (and have the family history to boot), I simply haven’t felt the need for one. And why not? For me personally, it primarily boils down to not wanting amphetamines, and there are a handful of reasons. But enough about me. I want to talk about just how weird our conceptualization of ADHD, and indeed, attention, are.
What is ADHD? Is it real?
ADHD, or attention deficit/hyper-activity disorder is a mental health condition so common that you’ve literally all heard of it, and many of you (assuming my readers are mostly just my friends) have diagnoses. For the purposes of this article, I’m going to mostly focus on adult (defined as 17+) ADHD. Childhood ADHD is diagnosed slightly differently. It has a strong correlation with adult ADHD, but sometimes people grow out of it, and sometimes adults grow into it.
ADHD is a modern epidemic. Over the last 20 years, the prevalence of ADHD has about doubled1. Most estimates place it at over 10% of the population, and it is considered to be even higher than that in the young generation that grew up with smartphones. However, like every mental health diagnosis, and perhaps more than most, ADHD diagnoses are often subject to skepticism.
Are we sure it isn’t just changes in diagnostic procedure?
This has been investigated a lot. The answer, as far as I can tell from perusing the literature, is yes, we are definitely sure. There’s a little bit of that, as the definition of ADHD has changed slightly2 between the DSM-IV and the DSM-V. (someone can now have both ASD and ADHD, which were not fully separated before) In addition, some college students trying to cram manage to fake it. But this is not nearly enough to explain the change we’ve seen. There are certainly more people who seem to be struggling with basic executive function today than 20 years ago.
How generational is it?
Certainly from looking at my peer group, it seems somewhat generational. Some of this may be a matter of perspective: I can think of a number of friends whose immigrant parents simply don’t believe in “mental health” at all. I think there’s something to learn there, but I’ll leave it for now. Anyone who has friends into Gen X may have noticed the difference. One friend is dating someone 8 years older than her, and she’s remarked how the minds of he and his friends are “just so much quieter” than her own peer group’s. But it’s not like ADHD was unheard of in older generations either.
So why the skepticism?
Well, because ADHD is a weird one.
ADHD and the Factors of Disease
In one of my favorite essays of all time3, Scott Alexander³, a Bay Area Psychiatrist with a Philosophy degree (and a Rationalist cult-celebrity), notes that what we consider a “disease” is a squishy cultural concept that is built of other pieces. He suggests that our intuitions of disease align with a short list of criteria. In Scott’s model, diseases are:
1. Something caused by the sorts of thing you study in biology: proteins, bacteria, ions, viruses, genes.
2. Something involuntary and completely immune to the operations of free will
3. Something rare; the vast majority of people don’t have it
4. Something unpleasant; when you have it, you want to get rid of it
5. Something discrete; a graph would show two widely separate populations, one with the disease and one without, and not a normal distribution.
6. Something commonly treated with science-y interventions like chemicals and radiation.
Scott suggests that classic diseases like cancer fulfill all of these criteria, but debated “conditions” like dwarfism, obesity, or (as is thankfully no longer in the DSM) homosexuality, fail some, but not all, of the criteria. I think it’s worth giving these criteria a look for ADHD. I’m going to cover them a little out of order.
Is ADHD Biological?
This one gets a little tricky for many mental health disorders, because psychology has, to date, very little basis in neuroscience. As a neuroscientist, I will self-servingly claim that this is mostly because neuroscience is extraordinarily difficult. The brain is incredibly complicated. Psychology, and by extension, most psychiatric diagnoses, are about predicting human behavior. We, in the scientific materialist reductionist frame, believe that human behavior is a result of the operations of the brain. However, the brain is a computer, and while we can model some of its low-level dynamics, we cannot look at a brain and predict much about a person’s behavior. Psychiatry is in the uncomfortable position of being part of a materialist medical tradition that attempts material manipulations (via pharmaceuticals), but does so based on diagnostics derived from psychology, which is ultimately a study of mind. So, ADHD is biological in theory, but we have no idea how.
There has been some attempt, in recent years, to find biomarkers of ADHD via functional neuroimaging. These attempts have been, on the surface, successful. They take scans of subjects either at rest or doing tasks, plug them through either the “resting state functional connectivity” mathematical paradigm or some kind of deep learning technique like below4, and can classify with some accuracy, whether a patient has ADHD.

This sort of study is cool enough, but they have major issues. First of all, ADHD is defined by behavior. The diagnostic tests are what the models are trained on. They do not get a particularly high predictive accuracy, though it is well-above statistically significant. So, why would we do a $600 brain scan to only semi-accurately predict how someone will score on a $5 test? Second, deep neural nets like the above (or functional connectivity analysis) tend to be extremely uninterpretable. If the purpose of doing the study was not to make a useful diagnostic tool, but instead to elucidate the mechanism of ADHD, these studies have entirely failed to do so. To me, studies like these reek of trying to add an authoritative air of “biologicalness” to an invented category without actually teaching us whether it is a good category. So is ADHD biological in the criteria #1 sense? At the absolute level, of course it’s biological. After all, I’m always reminding people,
The brain doesn’t cause the mind. The mind supervenes on the brain. They both cause each other.
Anything measurable in behavior can theoretically someday be read from the brain. But is ADHD demonstrably more biological than psychological traits we don’t think of as biological at all, like “generosity”, “laziness”, or “liking horses”? No, I don’t think so. Furthermore, there is so far no gene, no visible brain structure, and no chemical or hormonal abnormality that leads to ADHD. I think ADHD fails criteria #1.
Is ADHD Rare?
As stated in the intro, ADHD is not that rare these days. Sure, it’s not MOST people. But it’s a lot more common than most things we think of as disease. If one in every 5–10 people has some mental trait, is it really a disease? We’ll give it a “maybe” on criteria #3.
Is ADHD Discrete?
Nope, absolutely not. But I want to give this one a little bit of attention. How do we measure ADHD? The DSM-5 lists some criteria, but the DSM-5 is derived from research that looks at things in more detail. There are many ADHD screening instruments used for more rigorous research. The figure below5 shows a sample of a couple of them. These are images of probability distributions. The blue curve represents a sampled estimate of how people score on different ADHD tests. The red cutoff line is when someone has ADHD. As you can see, it’s a continuum. There are people who “really” have ADHD, a few more people who “sorta” have ADHD, and even more people who don’t have ADHD, but trend in that direction. The cutoff line is agreed upon in the research, but it is absolutely arbitrary.
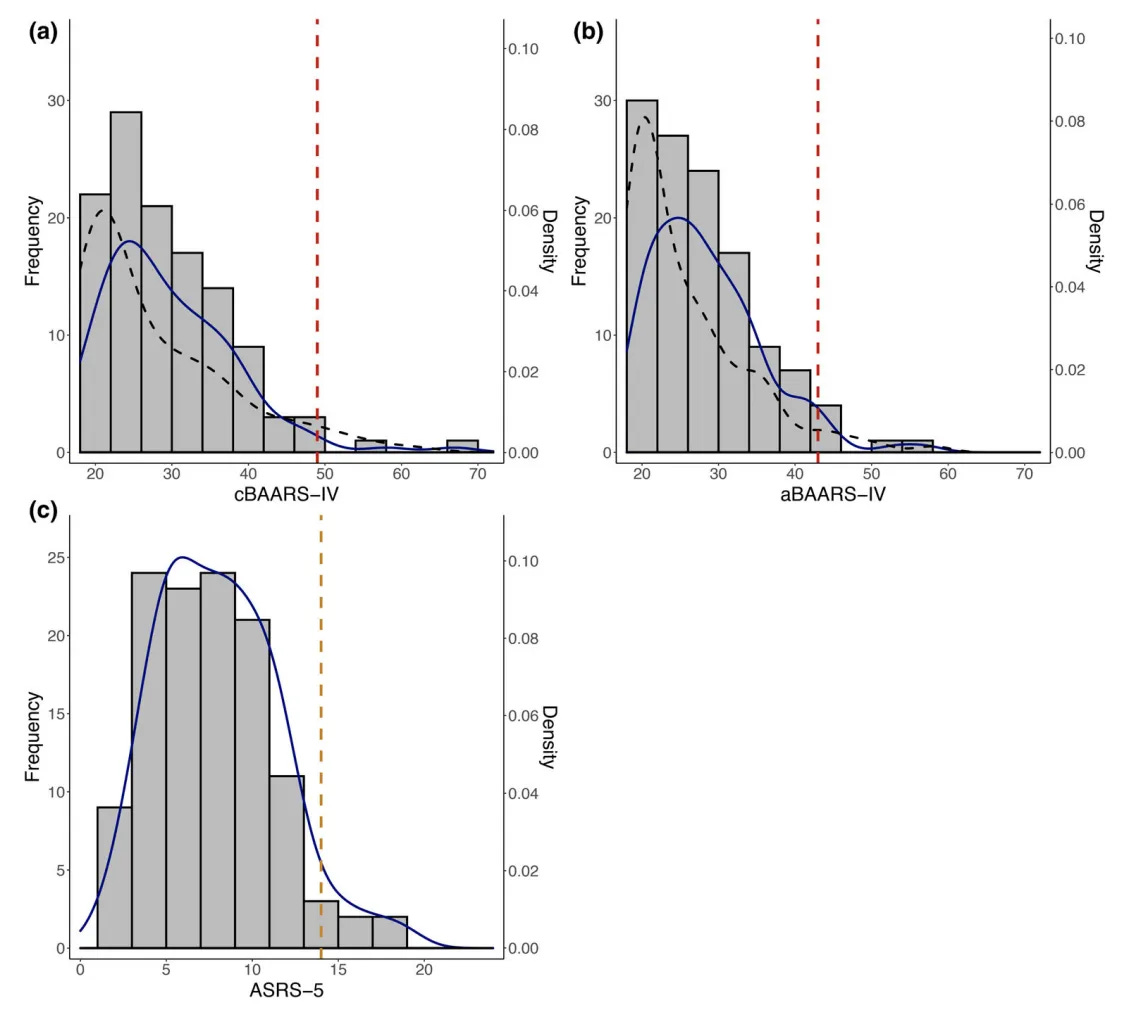
The study I cite above initially interested me because it also tried to break down how these same ADHD patients performed on different attentional tasks. There are a whole bunch of different words that the literature argues over for different sorts of attention and what they mean. “Attention” is itself a pretty squirrely concept. The hope of these researchers is that those pieces of attention can be broken down into much simpler tasks that can be tested psychophysically (i.e. with reaction times while doing simple tasks). These tasks consist of looking at dots or arrows doing different things, and reacting to them by pressing buttons. There are tons of variations:

To summarize this particular paper, the researchers were looking for differences between adult and child ADHD, and found that adults have more executive vigilance issues. Executive vigilance has to do with noticing details while being distracted by other things. The researchers also note that there is individual variation in the different attentional issues that different ADHD patients will have. I’ll talk more about attention later. But for now, criteria #5 is a strong no.
Is ADHD Treated With Sciencey Interventions?
Yes. To be precise, it is treated, but not cured. The main intervention is medication, and the medications are stimulants: usually amphetamines, especially for adult ADHD. But here’s the thing: amphetamines work on everyone. They increase energy, focus, and wakefulness. There is no evidence that amphetamines operate any differently between people with ADHD and those without. (I believe the story is a little more complicated with Ritalin) Amphetamines increase focus, and in our current game, focus is under demand. I’m not going to shame anyone for deciding to take them; it is a valid choice. However, just like the steroids of body-builders, they have many side effects. They can cause narcolepsy, heart issues, and memory issues. In short, like all stimulants, they are dependency-forming, and have a bit of a character of borrowing from the future. This is sort of a sciencey intervention, but a very generic one, that doesn’t discern between people with and without the condition. I’ll give it a weak yes for criteria #6.
Is ADHD Unpleasant?
This is another weird hole that several mental health conditions fall into, and it is the reason that we have terms like “neurodivergent” and “neurotypical” popping up. The leftist critical take6 has its standard form: runaway capitalism has created an environment that is stigmatizing a totally natural way to be in order to extract productivity from workers. I think leftist takes often tend to be somewhat correct, but have a rather violent and patronizing body of rhetoric that alienates people. They also tend to reify identification with traits that may in truth be pretty flexible.
Instead of playing into that rhetoric, I’ll note that ADHD is unpleasant, or people would not seek treatment. However, it is not unconditionally unpleasant, in the sense that depression, severe ASD (at least the stimulus sensitivity), Tay-Sachs, or PTSD is. One can imagine ADHD not really being a problem while in a fairly undistracted ancestral environment. How many of my friends with ADHD find it to be as taxing while backpacking, for example? It is also quite obvious that the need to do work with massive attentional demands is increasing greatly. Our economy is becoming increasingly competitive, and we constantly interact with phones, computers, timers, alerts, and advertisements, just to function in the world. Some of this makes having ADHD harder, and some of it likely reinforces, or even creates, ADHD behavioral patterns.
The Game is changing, and this is twice as true on college campuses, where the amphetamine black market is booming. Many ADHD-diagnosed students sell some of their prescription to other students on the side. From7:
Adderall and other stimulants, it turns out, are the perfect chemical accomplice in a society that prizes productivity above all else. We have entered what political theorist Wendy Brown describes as “a hyper-competitive order”, where “every human being is now required to understand themselves as a little bit of human capital”. What results is a kind of arms race in which young people feel they have to be on stimulants to compete with their drug-taking peers, or to pull the all-nighters demanded of them by elite institutions.
This sounds a LOT like the situation that the natty YouTube body-builders are complaining about. Want to compete at the top? You’ve gotta juice.
It is true that maybe the most disadvantaged students (those who struggle with attentional tasks enough to get an ADHD diagnosis) could use the boost even more. Desiring equity here makes sense. However, it’s worth remembering that the cutoff is arbitrary and amphetamines enhance everyone — at least at the task of frantic studying. Imagine that student A is very smart, prepared, and otherwise highly competitive, such that they’ll be able to land a job and care for themselves regardless, but they also qualify for an ADHD diagnosis. Are they more “deserving” of amphetamine enhancement than student B, who falls just on the other side of the ADHD line, but is struggling to not fail out, perhaps because they weren’t adequately prepared in high school? What if giving amphetamines to the student B instead of student A would mean they both can get jobs and pay rent, but giving them to A instead of B meant A would become an exec and B would fail out of school? Questions about “deserves” always fall apart at the seams if you look closely enough. Having bigger muscles might make my life easier. Do I deserve to juice more because I’m naturally lean?
Again, I don’t want to shame anyone for taking amphetamines (or juicing) in a way that helps improve their lives. I think this can be a reasonable and moral thing for an individual to do given the world they are handed. I’m looking at the broader societal and cultural picture here, and the effects of the incentive system we’ve created.
This section was long. I think I have to say “it’s complicated” for criteria #4.
Is ADHD Involuntary?
Well, like a good philosopher8 and good Buddhist, I don’t believe in free will at the end of the day. It’s all either nature or nurture (our karma), and we don’t choose either of those. It’s not “your mind versus your brain chemistry”. Your mind is your brain chemistry. Perhaps a better question to ask is, “is ADHD amenable to everyday decision-making and training regimens?”. It is at this point that I must bring meditation into the conversation.
Buddhist meditation is, among other things, like the attentional gym, as is clearly stated on the label. The 7th step of the Noble Eightfold Path is “Right Concentration”. While I must note Buddhism is not unique among religions to employ this tool, the association of meditation with Buddhism is iconic. In this tradition, the idea that meditation is a training technique that (among other things) can help one to concentrate on the right things in the rest of life is very clear¹. But if this is so obvious, why isn’t meditation recommended more as a treatment for ADHD? It has certainly helped me, to the degree that I find amphetamines, and even caffeine (unless I want to skip a midday nap in my 6am-10pm schedule), completely unnecessary. When I compare this to the YouTube body-builders, I have to ask,
In the “game” of focused productivity, are we prescribing steroids before ever going to the gym?
Well, that was the question that inspired this essay, and I looked into it. Let’s drop Scott’s list of criteria and just say ADHD is sort of like a disease and sort of not. If you go to a Doctor and say you have this dis-ease, you can get amphetamines pretty easily. If you work in finance, you can just buy cocaine from your most productive coworker instead. Do so if you want to, but be aware that all stimulants have plenty of side effects. Let’s now redirect our attention to the question of how much meditation can help ADHD.
Could Meditation be “The Gym” for Attention?
I have done a quick literature review, following the citation chain, and honestly…I’ve been disappointed by what I’ve found so far. There have been clinical investigations into the application of meditation to ADHD, but not many and not big ones! (Modesto-Lowe 2015)9, (Mitchell 2017)10, (Zhang 2018)11, and review (Zhang 2023)12 investigate such studies. These all report positive results versus controls, but the results are generally a little mild, and study sizes a little small. Given my own experience and that of friends, I was surprised to see the positive effects were so mild, until I saw the meditation protocols. Mindfulness meditation starting at 5 minutes a day and working up to 20?!? Get outta here, that’s nothing! Would you go to the gym for 5 minutes a day and expect any sort of change? 30–60 minute daily sits are table stakes for reaching “access concentration”, which is generally considered the first describable meditative benchmark.13
Mindfulness Awareness Practices for ADHD
There is a protocol of using meditation for ADHD in adults that has some momentum behind it, and it is used in many of these studies: The “Mindfulness Awareness Practices (MAPs) for ADHD program”. I looked into it. The intro book by Lidia Zylowska is free online as well. Ok, I’m going to need to speak a little carefully here. First, I want to say, this is a really noble effort. The people who put together this program have clearly put in enormous work to make something that is culturally accessible, motivating, and educational to ADHD. I have never run a clinical trial, and I know the effort and bureaucracy involved is enormous. That being said…I think this standard protocol suffers enormously from its disconnection from old meditative traditions. To my (limited) meditative experience, this protocol throws out about 90% of the power of the Buddha’s methods.
Throughout the book there’s occasional references to psychology studies, and lots of talk about “mindfulness” as a great new tool. This is all fine and good. Referencing studies can increase faith and motivation for a certain type of person, and mindfulness is indeed important. However, when I look at my own introduction to attention practice, via lineages of Theravada teachers and 2500-year old Pali suttas, I’ve gotta say…something was clearly lost in translation here. “Mindfulness” is but one of the 5-factors (pañcabalā) of awakening, in addition to faith, energy, wisdom, and concentration. There is no talk about how to sit for proper energy, nothing about wisdom, and perhaps critically, very little about concentration, in MAPs for ADHD. I understand (and Mitchell 201514 outright states) that part of the reason that the time is so low is because it’s hard to get ADHD people to do something for a long time every day. Well, to that I say that the possibility of liberating enlightenment is a lot more motivating than a study saying that following these practices led to a 10% improvement at such-and-such controlled task. The motivation itself is one of the things lost in the import of this material into the realm of clinical psychology.
“Meditation” Can Mean a Lot of Different Things
In my personal experience with meditation, the tendency to focus in everyday life is extremely plastic and amenable to meditative practice, but it must be the right kind of meditation. Just as how you’d quickly follow someone revealing they like “workouts” with “what kind of workout?”, hearing a recommendation for “meditation” should quickly be followed with “what type?”. In (Laukkonen 2023)15 and (Laukkonen 2021)16, the majority of the myriad forms of meditation are sorted into four (non-comprehensive) categories²:
Focused Attention (FA) meditation is when one maintains a focus on a particular aspect of experience to the exclusion of everything else. Good examples are the feeling of the breath at the tip of the nostrils, or the center of a candle flame.
Open Monitoring (OM) meditation is when one maintains a non-preferential awareness of everything happening in the present moment. This is what is often meant by “vipassanā” meditation. Sometimes, FA is used as a ramp to get into more powerful OM meditation. (as is done in the Jhanic Theravada technique I was taught)
Non-dual Awareness (ND) meditation is when one attempts to find the “ground of experience” that is neither perception nor non-perception, the thing that is always there regardless of the type of experience. There are several routes to this type of meditation, and some would consider it to be “the goal”.
Loving Kindness (LK) meditation sits in a strange place with surprisingly deep relation to all of the above types. It is related to mettā, the “first and last training of Buddhism”. One directs their attention towards the experience of compassion itself.
I believe these all represent workouts of various types with the attention. They are very general postures with respect to experience, and noticing and being able to activate these postures is undoubtedly powerful. FA and LK are often taught first. Before we can really inspect experience, we have to get the really distracting “stuff” out of the way. The MAPs approach looks a bit more like OM. Not only does this seem like a strange approach to me, like skipping the “leg day” of FA, but the times are too short. A teacher told me that one cannot really hope to get anywhere with concentration meditation (FA) sits of less than 45 minutes. To my experience, this has certainly been true. Sure, you have to build up a bit as you learn to sit well. Don’t sprain yourself. (it’s possible) But my most beneficial sits have been longer than 2 hours. In addition, the tendency to concentrate builds up over days. Consistency is important.
A brief distraction: What even IS “attention”?
To this point, I have avoided the particular wrinkle in all of this: that “attention” itself doesn’t have the cleanest definition. One neuroscientific view is that attention is a “top-down” something or other from the higher brain that modulates the representation of bottom-up stimulus in the field of perception. A pretty easy-to-understand example is investigated in (Çukur 2015)17, a paper from my grad school lab. The short is that when subjects are told to attend to a particular type of object, and shown stimulus, the space that that sort of object takes up in the brain is increased. It’s easier to show than tell. Luckily there’s an interactive viewer for this result if you’re interested.

However, this is only one of several types of things that researchers call attention. One can find spatial attention, temporal attention, selective attention (that’s the above study), inhibitory attention, internal attention, alerting, orienting, distraction, arousal vigilance, and executive vigilance all studied as different objects in the literature, and associated with different brain areas. (though Frey 201518 suggests some common underlying mechanisms) The more one looks into this, the more one sees that “attention”, as used in common speech, is nothing more or less is “the internal conditions that cause particular experiences to arise conditioned on whatever the previous state of the mind was”. In Buddhist phenomenology, this is very close to the entire function of the citta (the mind/heart), and meditation is all about conditioning the heart.
More Evidence Concerning Attention Tasks
If we step, for a moment, outside of the ADHD research, we can find more research on the effects of meditation on attention. Perhaps when unbound by the restrictions of clinical pilot studies, or a dependency on recruiting and maintaining the interest of subjects with ADHD, it’s a bit easier to experiment. There’s a pile of evidence19 suggesting that long-time meditators accumulate a variety of benefits related to attention, including alerting, executive control, inhibition, shifting and updating. There’s functional biomarkers that can distinguish meditators from non-meditators20 to about the same extent as can be done for those with or without ADHD21.
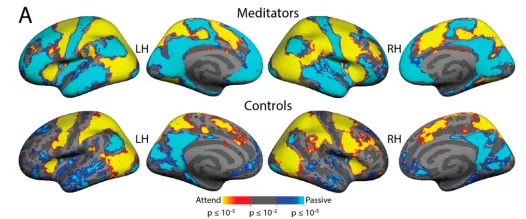
Does this demonstrate that meditation can cure ADHD? Not quite, but it suggests that long-term meditative practice can have dramatic and long-lasting effects on the brain, in exactly the ADHD problem areas.
Closing Thoughts
For now, I’m going to wrap this essay up, as I feel my mind pulling me on to other projects. The study of attention is complex. It’s not always quite clear what is being referred to, or what is damaged or underdeveloped in ADHD, if anything. I’ll throw in that I have heard it said that an Arhat (one who has attained the 4th and final stage of enlightenment in Theravada Buddhism) no longer believes that there is any such thing as “attention”, and that this is an important difference between the 3rd and 4th stage. If one perceives no attention, I suppose that one cannot be bothered by any sort of “Attention Deficit”. There, I solved it. The cure to ADHD is complete enlightenment!
More seriously, I worry that our unreasonable society is in a place where competition is forcing us to place our attentions under greater and greater demand, and this is forcing us to medicate. It’s cocaine and finance all over again, but everywhere. Again, I do not blame anyone for using amphetamines. But it is strange to me that we turn to drugs without ever going to the meditative gym. If you have ADHD maybe try it out? And hey, at least in weightlifting, steroids AND the gym are known to produce much better effects than steroids alone, so it seems worth investigation even if the speed is working for you. I also worry that the way meditation is being clinically investigated is drawing conclusions after administering some kind of weak, watered-down, meditative technique. Can we get some real Dhamma teachers to develop those protocols and oversee their administration? If you want to start meditation, there are tons of great resources. I would recommend some of the extremely accessible Buddhist resources like Right Concentration, by Leigh Brasington22, or Mastering the Core Teachings of the Buddha, by Daniel Ingram way before any of these clinically-approved manuals. That being said, if you made it to the end of this essay, your attentive abilities are already top-notch!
Footnotes
¹”Right Concentration” means many things beyond this, and refers quite specifically to Jhanas in some places, but that is a topic for another essay.
² I will note that (Laukkonen 2021) is fantastic and available online for free.
³Scott Alexander’s real last name is “Siskind”. There was a whole drama about it a couple years ago, but rest assured, he’s a real Doctor.
Citations
Abdelnour E, Jansen MO, Gold JA. ADHD Diagnostic Trends: Increased Recognition or Overdiagnosis? Mo Med. 2022 Sep-Oct;119(5):467–473. PMID: 36337990; PMCID: PMC9616454.
Epstein, Jeffery N., and Richard E. A. Loren. 2013. “Changes in the Definition of ADHD in DSM-5: Subtle but Important.” Neuropsychiatry 3 (5): 455–58.
Mao, Zhenyu, Yi Su, Guangquan Xu, Xueping Wang, Yu Huang, Weihua Yue, Li Sun, and Naixue Xiong. 2019. “Spatio-Temporal Deep Learning Method for ADHD fMRI Classification.” Information Sciences 499 (October): 1–11.
Coll-Martín, Tao, Hugo Carretero-Dios, and Juan Lupiáñez. 2021. “Attentional Networks, Vigilance, and Distraction as a Function of Attention-Deficit/hyperactivity Disorder Symptoms in an Adult Community Sample.” British Journal of Psychology 112 (4): 1053–79.
Chapman, Robert. Empire of Normality: Neurodiversity and Capitalism. 1st ed., Pluto Press, 2023.
Lucas, Catherine. 2018. “Going off-Label.” The Lancet Child & Adolescent Health 2 (8): 556.
Strawson, Galen, and Gary Watson. “Free will.” Routledge encyclopedia of philosophy. London: Routledge (1998).
Modesto-Lowe, Vania, Pantea Farahmand, Margaret Chaplin, and Lauren Sarro. 2015. “Does Mindfulness Meditation Improve Attention in Attention Deficit Hyperactivity Disorder?” __World Journal of Psychiatry__ 5 (4): 397–403.
Mitchell, John T., Elizabeth M. McIntyre, Joseph S. English, Michelle F. Dennis, Jean C. Beckham, and Scott H. Kollins. 2017. “A Pilot Trial of Mindfulness Meditation Training for ADHD in Adulthood: Impact on Core Symptoms, Executive Functioning, and Emotion Dysregulation.” Journal of Attention Disorders 21 (13): 1105–20.
Zhang, Junhua, Amparo Díaz-Román, and Samuele Cortese. 2018. “Meditation-Based Therapies for Attention-Deficit/hyperactivity Disorder in Children, Adolescents and Adults: A Systematic Review and Meta-Analysis.” Evidence-Based Mental Health 21 (3): 87–94.
Zhang, Zeping, Xiaolong Chang, Weijing Zhang, Suyong Yang, and Guangsheng Zhao. 2023. “The Effect of Meditation-Based Mind-Body Interventions on Symptoms and Executive Function in People With ADHD: A Meta-Analysis of Randomized Controlled Trials.” Journal of Attention Disorders 27 (6): 583–97.
Ingram, D. (2018). Mastering the Core Teachings of the Buddha: An Unusually Hardcore Dharma Book. United Kingdom: Aeon Books
Mitchell, John T., Lidia Zylowska, and Scott H. Kollins. 2015. “Mindfulness Meditation Training for Attention-Deficit/Hyperactivity Disorder in Adulthood: Current Empirical Support, Treatment Overview, and Future Directions.” Cognitive and Behavioral Practice 22 (2): 172–91.
Laukkonen, Ruben E., Matthew D. Sacchet, Henk Barendregt, Kathryn J. Devaney, Avijit Chowdhury, and Heleen A. Slagter. 2023. “Chapter 4 — Cessations of Consciousness in Meditation: Advancing a Scientific Understanding of Nirodha Samāpatti.” In Progress in Brain Research, edited by Tal Dotan Ben-Soussan, Joseph Glicksohn, and Narayanan Srinivasan, 280:61–87. Elsevier.
Laukkonen, Ruben E., and Heleen A. Slagter. 2021. “From Many to (n)one: Meditation and the Plasticity of the Predictive Mind.” Neuroscience and Biobehavioral Reviews 128 (September): 199–217.
Çukur, Tolga, Shinji Nishimoto, Alexander G. Huth, and Jack L. Gallant. 2013. “Attention during Natural Vision Warps Semantic Representation across the Human Brain.” Nature Neuroscience 16 (April): 763.
Frey, Julia Natascha, Philipp Ruhnau, and Nathan Weisz. 2015. “Not so Different after All: The Same Oscillatory Processes Support Different Types of Attention.” Brain Research 1626 (November): 183–97.
Sumantry, David, and Kathleen E. Stewart. 2021. “Meditation, Mindfulness, and Attention: A Meta-Analysis.” Mindfulness 12 (6): 1332–49.
Devaney, Kathryn J., Emily J. Levin, Vaibhav Tripathi, James P. Higgins, Sara W. Lazar, and David C. Somers. 2021. “Attention and Default Mode Network Assessments of Meditation Experience during Active Cognition and Rest.” Brain Sciences 11 (5). https://doi.org/10.3390/brainsci11050566.
Sutcubasi, Bernis, Baris Metin, Mustafa Kerem Kurban, Zeynep Elcin Metin, Birsu Beser, and Edmund Sonuga-Barke. 2020. “Resting-State Network Dysconnectivity in ADHD: A System-Neuroscience-Based Meta-Analysis.” The World Journal of Biological Psychiatry: The Official Journal of the World Federation of Societies of Biological Psychiatry 21 (9): 662–72.
Brasington, L. (2015). Right Concentration: A Practical Guide to the Jhanas. United States: Shambhala
Very thorough analysis, great job!